 |
Research Article
Prevalence of hypertension among adolescents living with human immunodeficiency virus in Lagos, Nigeria
1 Consultant Paediatrician/Deputy Director of Research, Clinical Sciences Department, Nigerian Institute of Medical Research, Yaba, Lagos, Nigeria
2 Senior Research Fellow, Clinical Sciences Department, Nigerian Institute of Medical Research, Yaba, Lagos, Nigeria
3 Principal Medical Officer, Clinical Sciences Department, Nigerian Institute of Medical Research, Yaba, Lagos, Nigeria
4 Senior Medical Officer, Clinical Sciences Department, Nigerian Institute of Medical Research, Yaba, Lagos, Nigeria
5 Biostatistician/ Medical Officer, Clinical Sciences Department, Nigerian Institute of Medical Research, Yaba, Lagos, Nigeria
6 Medical Officer, Clinical Sciences Department, Nigerian Institute of Medical Research, Yaba, Lagos, Nigeria
7 Lecturer/Nutritionist, Federal College of Education (Technical) Akoka, Lagos, Nigeria
8 Consultant Paediatrician/Research Fellow, Clinical Sciences Department, Nigerian Institute of Medical Research, Yaba, Lagos, Nigeria
Address correspondence to:
Odubela Oluwatosin O
MBChB, MScPH, 6 Edmond Crescent, Yaba, Lagos,
Nigeria
Message to Corresponding Author
Article ID: 100009P05DN2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
David AN, Gbaja-Biamila TA, Odubela OO, Musari-Martins TE, Ezemelue PN, Opaneye BA, Lagunju MM, Arije DM, Abubakar RA, Ezechi LO, Salako AO. Prevalence of hypertension among adolescents living with human immunodeficiency virus in Lagos, Nigeria. Edorium J Pediatr 2021;5:100009P05DN2021.ABSTRACT
Aims: This study sought to evaluate the prevalence of hypertension and its associated factors among adolescents living with human immunodeficiency virus (HIV) in Lagos, Nigeria.
Methods: A cross-sectional study involving adolescents attending an antiretroviral therapy (ART) clinic in Lagos was enrolled in the study. Case record form was developed to capture data on socio-demographic, clinical, laboratory, and treatment parameters of Participants. Blood pressure readings, waist circumference, and fasting lipid profiles of participants were also obtained. Hypertension was defined as a blood pressure reading ≥95th percentile for age, sex, and height or readings above 120/80 mmHg irrespective of age or gender by the Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents.
Results: One hundred and fifty-three adolescents participated in the study with males accounted for 52% of the study population. The majority of participants were in secondary school (79.7%), had both parents alive (73.2%), and acquired HIV infection through vertical transmission (99.3%). The prevalence of hypertension was 10.5%. The predictive risk factors for hypertension were older age [odds ratio (OR) 1.557, 95% confidence interval (CI) 0.344–7.040], waist circumference (OR 6.435, 95% CI 1.396–29.666), duration on ART >8 years (OR 1.308, 95% CI 0.332–5.153), and dyslipidemia (OR 2.942, 95% CI 0.726–11.914). However, only waist circumference was statistically significantly associated with hypertension (p < 0.05).
Conclusion: Our study revealed a high prevalence of hypertension among adolescents living with HIV. There is a need for regular monitoring of blood pressure and associated risk factors during routine care.
Keywords: Adolescents, Blood pressure, HIV, Hypertension, Lagos
INTRODUCTION
Sub-Saharan Africa (SSA) accounts for over two-thirds of the global burden of human immunodeficiency virus (HIV) [1], and approximately 85% of the 1.8 million adolescents living with the disease are in the sub-region [1],[2],[3]. This increasing population of adolescents living with HIV in the sub-region is in part due to the success of highly active antiretroviral therapy (HAART), which has enabled perinatally infected children to survive into adolescence and adulthood. Adolescents and young people (aged 15–24 years) also account for a significant proportion of new HIV infections, thus increasing the burden of HIV among adolescents. In 2019, about 170,000 adolescents acquired HIV infection, majority of them in low-and middle-income countries, including those in SSA [4]. Nigeria, the most populous nation in Africa, bears the second largest burden of the global HIV epidemic and has one of the highest rates of new infections in sub-Saharan Africa. However, this increased longevity is associated with an increasing prevalence of co-morbidity with various non-communicable diseases (NCDs) [3],[4],[5]. This could portend a detrimental impact on the overall gains of HIV care, considering its long latency period, prolonged course, and associated functional impairment and disability [5],[6],[7].
Apart from the burden of HIV and its detrimental effect on the African population, the continent is also the most affected region with the rapidly increasing burden of hypertension and other NCDs [8]. The prevalence of hypertension in Nigeria forms a substantial proportion of the total burden in Africa because of her large population [9],[10].
Hypertension remains the leading cause of premature death and a predominant risk factor for all forms of cardiovascular-related morbidity and mortality [8]. Globally 1 in 7 persons are hypertensive with approximately 17 million cardiovascular-related deaths recorded in 2016 [11]. This has prompted the World Health Organization (WHO) to initiate measures to reduce the prevalence of the “silent killer” by 25% by the year 2025 [8].
Hypertension in children and adolescents is becoming an increasing public health concern because evidence shows that the disease tracks from childhood to adulthood [12],[13]. Hypertension in the pediatric population is associated with immediate adverse effects on cardiovascular structure and function, neurocognitive function, and also serves as a marker for subclinical atherosclerosis in adulthood [14],[15].
A systematic review reported a global hypertension prevalence of 4% among children below the age of 19 years. This is comparable to the 5.5% reported among African children and adolescents [13] and 4% among Nigerian children [12]. This shows that hypertension is relatively common in children and adolescents. Thus, the need for pediatric health care practitioners is to evaluate blood pressure regularly in routine clinical practice.
Adolescents living with HIV (ALHIV) could further be predisposed to hypertension and its sequelae of cardiovascular disease, disability-adjusted life-years, and mortality as a consequence of prolonged HIV infection and ART. The mechanism of onset of hypertension and in people living with HIV (PLHIV) is multifactorial involving the primarily modifiable and non-modifiable risk factors, as well as the (in)direct effect of HIV/ART resulting in chronic inflammation, lipodystrophy syndromes, premature ageing of the cardiovascular system, and renovascular injury among others [5],[6],[7][16],[17],[18]. In a retrospective unpublished review of blood pressure readings of children and adolescents living with HIV in our facility, we recorded a prevalence of 7%. In contrast, a higher prevalence of 25–45% for hypertension has been reported among adults living with HIV with associated increased complications and poor life expectancy in addition to the high cost of living [19],[20].
To address this alarming burden of hypertension, a “silent killer” among adults living with HIV, there is a need to monitor children and adolescents living with HIV to promptly identify, treat, and prevent the sequelae of hypertension in adulthood. However, there are limited reports on hypertension in children and adolescents living with HIV in our sub-region. This study aims to evaluate the prevalence of hypertension and its associated factors among adolescents living with HIV in Lagos, Nigeria.
MATERIALS AND METHODS
This was a cross-sectional study among adolescents attending the ART clinic at the Clinical Sciences Department of the Nigerian Institute of Medical Research, Yaba, Lagos. Adolescents (aged 10–19 years) living with HIV on antiretroviral drugs for at least six months and who consented (consent ± assent) to participate in the study were enrolled. Adolescents living with HIV with significant co-morbidities such as cerebral palsy, seizure disorders, sickle cell anemia, or other chronic illness and those with acute illness were excluded from the study.
A case record form (CRF) was developed to collect data on socio-demographic, clinical, laboratory, and antiretroviral treatment parameters of participants. Socio-demographic information included age, gender, education, occupation, ethnicity, and socioeconomic status (determined by parental education and occupation). The age at HIV diagnosis, time of commencement of ART, duration on ART, previous and current antiretroviral regimen, family history of hypertension, and current (within the last six months) Cluster of Differentiation 4 Lymphocyte (CD4) counts and HIV viral load were obtained from the clinic database. The weight (in kilograms) and height (in centimeters) were obtained with the combination scale and stadiometer (Seca Hamburg Germany, Model 786 2021994) with the participants in light clothing and barefoot. Waist circumference (in centimeters) was obtained with a non-stretchable medical tape rule applied horizontally at the level of the participant’s umbilicus. The height was converted to meters and the body mass index (kilograms per square meter) calculated using the standard formula. The age and sex-adjusted z scores and percentiles of these anthropometric measures were obtained from WHO standard growth charts for children and adolescents.
Two blood pressure readings were obtained 20 minutes apart, using an electronic sphygmomanometer Omron M3 Intellisense, Model: M3 (HEM-7131-E) (Omron Healthcare Co. Ltd) with the participant comfortably seated with the right arm (from which the blood pressure was obtained) placed at the level of the participant’s heart. The mean of the two readings was recorded as the participant’s blood pressure. If a high reading was obtained, a third measurement was conducted after another 20 minutes. The mean of the two closest readings was taken as the participant’s blood pressure. Point hypertension was defined as a blood pressure reading of ≥95th percentile for age, sex, and height or readings above 120/80 mmHg irrespective of age or gender [21].
After a 12-hour fast, approximately 6 mL of venous blood was collected from the antecubital fossa of each participant into plain vacutainer bottles. This was used to determine the fasting lipid profiles [total cholesterol, high-density lipoprotein cholesterol (HDL), low-density lipoprotein cholesterol (LDL), and triglycerides] using Roche C311 Clinical Chemistry autoanalyzer. Normal reference values for the lipids for adolescents were obtained from the National Cholesterol Education Program (NCEP).
Follow-up Plan: Results were communicated to all study participants and those with high blood pressure readings were referred to our hypertension clinic for further evaluation.
Data Analysis: Collected data was recorded, validated, and analyzed using the Statistical Package for Social Sciences (SPSS) software version 23. Descriptive and inferential statistics were applied in the course of the analysis. Descriptive statistics such as mean and standard deviation for normally distributed variables or median and interquartile range for skewed data were used to summarize continuous variables, while proportions were used to summarize categorical data.
Ethical approval was obtained from the Institutional Review Board (IRB) of NIMR, Lagos, before commencement of the study. Confidentiality was maintained, while voluntariness and freedom to withdraw at any point without negative consequences were emphasized before enrolment.
RESULTS
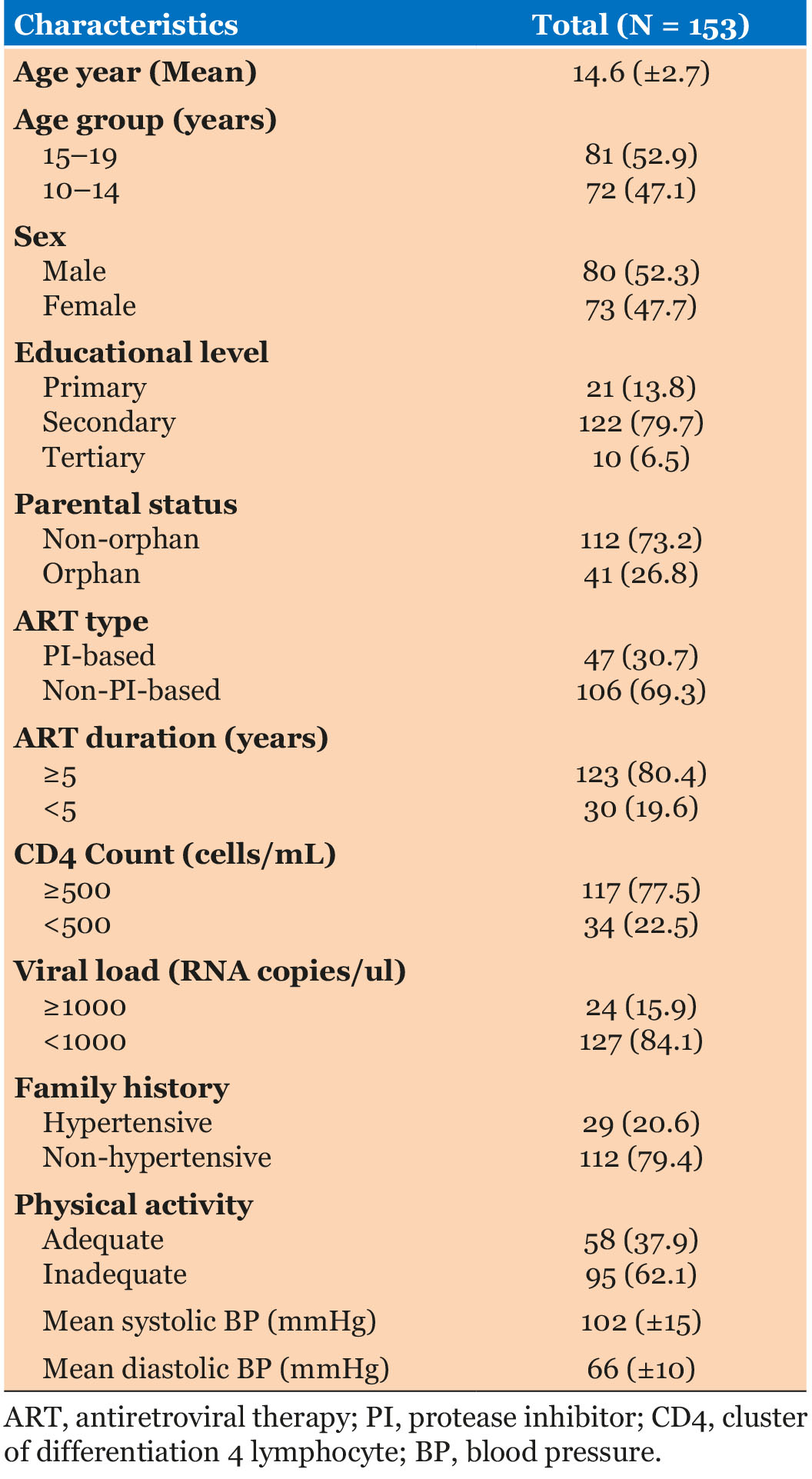
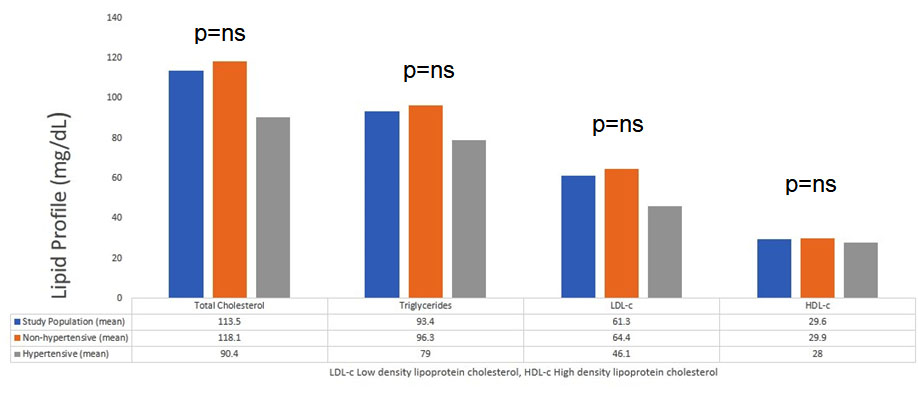
Out of the 153 adolescents living with HIV, who participated in this study, 80 were males and 73 were females, giving a male to female ratio of 1:0.9, and the mean age was 14.6 ± 2.7 years. A majority of the participants were in secondary school (79.7%), had both parents alive (73.2%), and belonged to the middle and lower socio-economic groups (83.7%). Most participants (99.3%) acquired the infection through vertical transmission. The median age [interquartile range (IQR)] at HIV diagnosis was 48 (24–84) months while the median duration (IQR) on ART was 9 (6–11) years. The mean systolic and diastolic blood pressures (± SD) of study participants were 102(±15) and 66(±10) mmHg respectively (Table 1). The mean lipid profile of study participants is depicted in Figure 1.
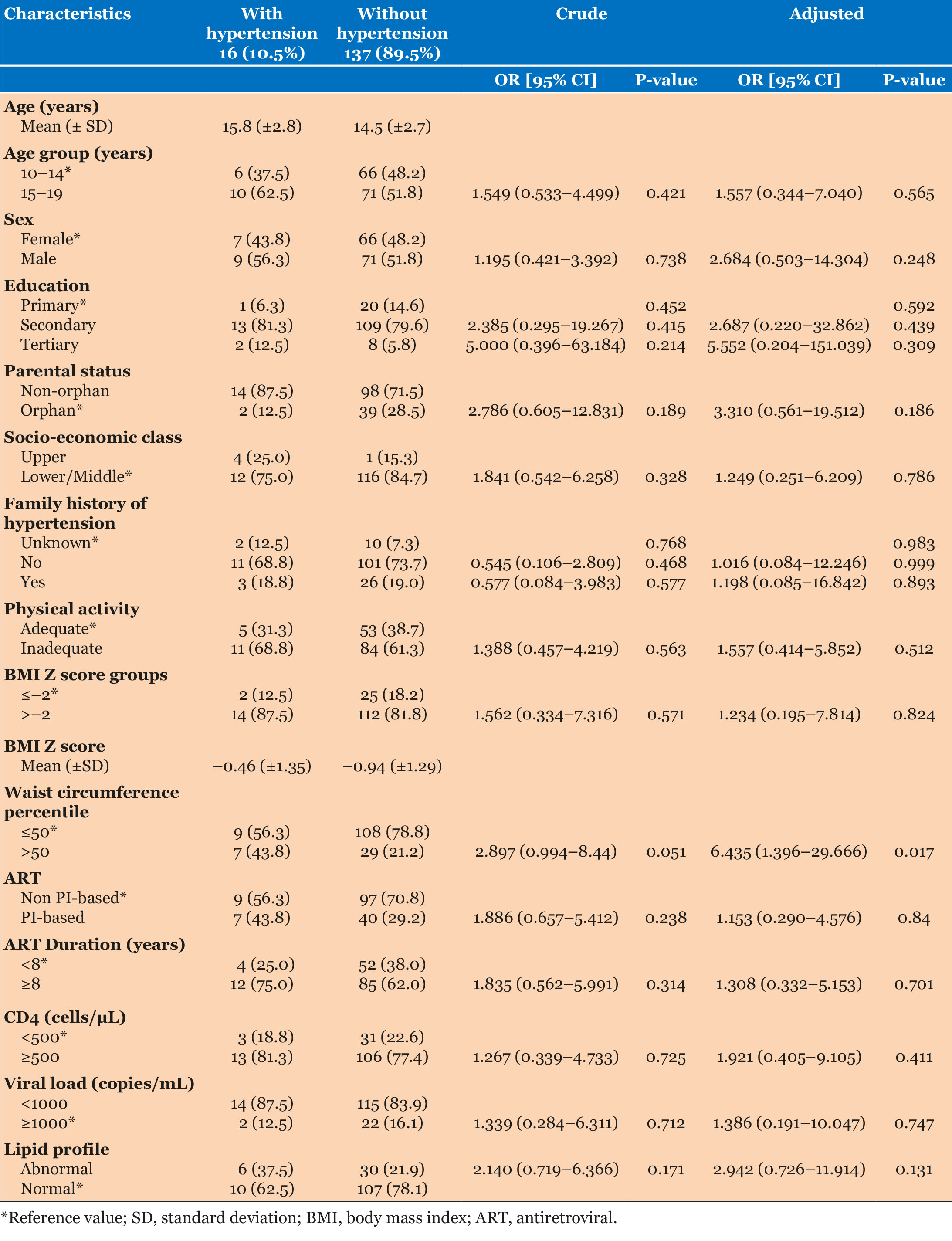
Sixteen participants (9 males and 7 females) had raised blood pressure readings, giving a prevalence of point hypertension among the study population of 10.5%. There were seven cases of diastolic hypertension, five cases of systolic hypertension, and four cases of both systolic and diastolic hypertension. The mean (± SD) readings for participants with hypertension was 125.1 (±11.3) mmHg and 83.4 (±7.7) mmHg for systolic and diastolic blood pressures, respectively, compared to 99.8 (±12.4) mmHg and 63.7 (±8.1) mmHg for those with normal blood pressure. Participants with hypertension were more likely to be older (15–19 years) [crude odds ratio (COR) 1.549, 95% CI = 0.533–4.499; adjusted odds ratio (AOR) 1.557, 95% CI = 0.344–7.040)] (Table 2).
Concerning the clinical and lifestyle characteristics, participants with hypertension were significantly more likely to have a waist circumference ≥50th percentile than those with normal blood pressure [COR 2.897, 95% CI = 0.994–8.44; AOR 6.435, 95% CI = 1.396–29.666]. Patients on protease inhibitor (PI)-based ART regimen [COR 1.886, 95% CI = 0.657–5.412; AOR 1.153, 95% CI = 0.290–4.576] and on ART > 8 years [COR 1.835, 95% CI = 0.562–5.991; AOR 1.308, 95% CI = 0.332–5.153] were more likely to have hypertension. Participants with hypertension had a higher likelihood of having at least one abnormal lipid profile [hypertriglyceridemia and/or low high-density lipoprotein (HDL)] than those without (COR 2.140, 95% CI = 0.719–6.366; AOR 2.942, 95% CI = 0.726–11.914). There was no statistically significant difference in family history of hypertension, level of physical activity, and duration on antiretroviral therapy among participants (Table 2).
DISCUSSION
Hypertension in adulthood is believed to track from childhood and adolescence. The onset of hypertension in PLHIV could be identified early in adolescence; thus, measures instituted to curtail its emergence and complications in this age group would save costs and lives.
In this study, the prevalence of hypertension among the participants was 10.5% with mean systolic and diastolic blood pressures of 125.1 (±11.3) mmHg and 83.4 (±7.7) mmHg, respectively. Most of the hypertensive ALHIV were on non-PI-based regimen and had been on ART for more than eight years.
The prevalence of hypertension among ALHIV in this study of 10.5% is higher than the pooled prevalence of 4% among the general pediatric population in Nigeria and globally [12],[22]. The high prevalence could be as a result of the effect of HIV/ART and chronic inflammation on the cardiovascular system among ALHIV. Our prevalence is comparable to 9.0% by Amadi et al. [23], 10.5% by Uwaezuoke et al. [24], 12.5% by Ajayi et al. [25] in Nigeria, and 9.0% by Cho and Kim [26] in Korea, but higher than the reported prevalence in 3.0% by Ibrahim et al. [27], 6.3% by Ezeudu et al. [28], and 7.0% by Akinbodewa et al. [29] in Nigeria. However, our finding is lower compared to reported prevalence in Houston, USA (15%), Chennai, India (21.5%), and Greece (23%) [25],[30],[31],[32]. Although most of these studies adopted the Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents [21]. These variations could be due to genetic factors, the difference in lifestyle, diets, study location, methodology, and underlying childhood obesity.
There was no significant difference between males and females in the prevalence of hypertension. This finding is in concordance with recent meta-analysis on the prevalence of hypertension in Nigeria and African pediatric population, buttressing the fact that gender appears to play little or no role in the prevalence of hypertension among children and adolescents [12],[13].
In the current work, none of our study participants with hypertension was obese. This could plausibly be alluded to HIV-infected children and adolescents being smaller and thinner than uninfected children of the same age and gender. In addition, the low socioeconomic status of most families in sub-Saharan Africa makes obesity uncommon [33]. This finding is contrary to reports among the general pediatric population where obesity was significantly associated with hypertension [12],[13],[22].
Waist circumference >50th percentile and dyslipidemia was predictive of being hypertensive in this study. This finding agrees with previous studies that have shown waist circumference and dyslipidemia are predictors of hypertension and other cardiovascular diseases [34],[35],[36],[37].
The prolonged ART and PI-based regimen were also positively correlated to the development of hypertension. This affirms the direct or indirect of ART resulting in chronic inflammation, lipodystrophy syndromes, and premature ageing of the cardiovascular system [16],[17],[18].
In this study, hypertension was not significantly associated with physical activity, family history of hypertension, duration, and type of ART. None of the participants were associated with a family history of hypertension which is similar to reports in Sudan and Nigeria [38],[39]. However, contrary reports by Sarfo et al. [39] and Sundar et al. [31] showed a positive association between family history and adolescent hypertension in Tobago and India, respectively. The predisposing factors to hypertension remain multifactorial beyond the effects of body mass index (BMI) and family history of hypertension [12].
To our knowledge, this is the first paper to highlight the prevalence of hypertension among adolescents living with HIV in sub-Saharan Africa. The high prevalence of hypertension among ALHIV in our setting reaffirms the need to ensure regular monitoring of blood pressure in the routine clinical care in ALHIV. This will assist in prompt detection, and appropriate management to mitigate the long-term debilitating effect of hypertension.
This study is limited by the cross-sectional nature of the study, the point prevalence of hypertension studied among participants and the number of participants included in the study. However, our findings show the need for further research to understand the pathophysiology of hypertension in this cohort.
CONCLUSION
Our study revealed a high prevalence of hypertension among ALHIV with waist circumference >50th percentile, dyslipidemia, long duration on ART, and PI-based regimen as predictive factors. This emphasizes the need for clinicians caring for ALHIV to institute comprehensive clinical services for prompt diagnosis of hypertension, cardiovascular diseases, and other metabolic disorders.
REFERENCES
1.
Miles To Go: Closing Gaps, Breaking Barriers, Righting Injustices: Global AIDS Update 2018. Geneva, Switzerland: UNAIDS 2018.

2.
Global and Regional Trends. 2019. [Available at: https://data.unicef.org/topic/hivaids/global-regional-trends/]
3.
Mahy M. Latest Estimates for Pediatric and Adolescent HIV Prevalence and Coverage. Geneva: UNAIDS; 2017. [Available at: http://regist2.virologyeducation.com/2017/9HIVped/01_Mahy.pdf]
4.
Adolescent HIV prevention. 2020. [Available at: https://data.unicef.org/topic/hivaids/adolescents-young-people/]
5.
Overview of NCD’s and Related Risk Factors. Atlanta, GA: Centers for Disease Control and prevention (CDC); 2013.
6.
Noncommunicable diseases. 2019. [Available at: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases]
7.
Adolescent Health The Missing Population in Universal Health Coverage. 2018. [Available at: https://www.who.int/pmnch/media/news/2018/Adolescent-Health-Missing-Population-in-UHC.pdf?ua=1]
8.
Hypertension. 2019. [Available at: https://www.who.int/news-room/fact-sheets/detail/hypertension]
9.
Adeloye D, Basquill C, Aderemi AV, Thompson JY, Obi FA. An estimate of the prevalence of hypertension in Nigeria: A systematic review and meta-analysis. J Hypertens 2015;33(2):230–42. [CrossRef]
[Pubmed]
10.
Akinlua JT, Meakin R, Umar AM, Freemantle N. Current Prevalence Pattern of Hypertension in Nigeria: A Systematic Review. PLoS One 2015;10(10):e0140021. [CrossRef]
[Pubmed]
11.
Cardiovascular diseases (CVDs). 2017. [Available at: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds)]
12.
Ejike CECC. Prevalence of hypertension in Nigerian children and adolescents: A systematic review and trend analysis of data from the past four decades. J Trop Pediatr 2017;63(3):229–41. [CrossRef]
[Pubmed]
13.
Noubiap JJ, Essouma M, Bigna JJ, Jingi AM, Aminde LN, Nansseu JR. Prevalence of elevated blood pressure in children and adolescents in Africa: A systematic review and meta-analysis. Lancet Public Health 2017;2(8):e375–86. [CrossRef]
[Pubmed]
14.
Juhola J, Magnussen CG, Berenson GS, et al. Combined effects of child and adult elevated blood pressure on subclinical atherosclerosis: The International Childhood Cardiovascular Cohort Consortium. Circulation 2013;128(3):217–24. [CrossRef]
[Pubmed]
15.
Urbina EM, Lande MB, Hooper SR, Daniels SR. Target Organ Abnormalities in Pediatric Hypertension. J Pediatr 2018;202:14–22. [CrossRef]
[Pubmed]
16.
Mondy KE. Determinants of endothelial function in human immunodeficiency virus infection: A complex interplay among therapy, disease, and host factors. J Cardiometab Syndr 2008;3(2):88–92. [CrossRef]
[Pubmed]
17.
Trayhurn P, Wood IS. Adipokines: Inflammation and the pleiotropic role of white adipose tissue. Br J Nutr 2004;92(3):347–55. [CrossRef]
[Pubmed]
18.
Arpadi SM, Cuff PA, Horlick M, Wang J, Kotler D. Lipodystrophy in HIV-infected children is associated with high viral load and low CD4+-lymphocyte count and CD4+-lymphocyte percentage at baseline and use of protease inhibitors and stavudine. J Acquir Immune Defic Syndr 2001;27(1):30–4. [CrossRef]
[Pubmed]
19.
Xu Y, Chen X, Wang K. Global prevalence of hypertension among people living with HIV: A systematic review and meta-analysis. J Am Soc Hypertens 2017;11(8):530–40. [CrossRef]
[Pubmed]
20.
Ryscavage P, Still W, Nyemba V, Stafford K. Prevalence of systemic hypertension among HIV-infected and HIV-uninfected young adults in Baltimore, Maryland. South Med J 2019;112(7):387–91. [CrossRef]
[Pubmed]
21.
US Department of Health and Human Services, National Institutes of Health and National Heart, Lung, and Blood Institute. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents, NIH Publication. 2005. [Available at: https://www.nhlbi. nih.gov/files/docs/resources/heart/hbp_ped.pdf]
22.
Song P, Zhang Y, Yu J, et al. Global prevalence of hypertension in children: A systematic review and meta-analysis. JAMA Pediatr 2019;173(12):1–10. [CrossRef]
[Pubmed]
23.
Amadi OF, Okeke IB, Ndu IK, et al. Hypertension in children: Could the prevalence be on the increase? Niger Med J 2019;60(5):256–61. [CrossRef]
[Pubmed]
24.
Uwaezuoke SN, Okoli CV, Ubesie AC, Ikefuna AN. Primary hypertension among a population of Nigerian secondary school adolescents: Prevalence and correlation with anthropometric indices: A cross-sectional study. Niger J Clin Pract 2016;19(5):649–54. [CrossRef]
[Pubmed]
25.
Ajayi IO, Soyannwo MAO, Asinobi AO, Afolabi NB, Ayede AI, Bamgboye EA. Blood pressure pattern and hypertension related risk factors in an urban community in Southwest Nigeria: The Mokola hypertension initiative project, Ibadan, Nigeria. J Public Health Epidemiol 2017;9(4):51–64. [CrossRef]
26.
Cho H, Kim JH. Secular trends in hypertension and elevated blood pressure among Korean children and adolescents in the Korea National Health and Nutrition Examination Survey 2007–2015. J Clin Hypertens (Greenwich) 2020;22(4):590–7. [CrossRef]
[Pubmed]
27.
Ibrahim OR, Afolabi JK, Adedoyin AT, Ojuawo AI. Prevalence and risk factors for hypertension among school children in Ilorin, Northcentral Nigeria. J Fam Community Med 2019;26(3):181–6. [CrossRef]
[Pubmed]
28.
Ezeudu CE, Chukwuka JO, Ebenebe JC, Igwe WC, Egbuonu I. Hypertension and prehypertension among adolescents attending secondary schools in urban area of South-East, Nigeria. Pan Afr Med J 2018;31:1–9. [CrossRef]
[Pubmed]
29.
Akinbodewa AA, Adejumo AO, Lamidi OA, Adeyemi O. Clustering of cardiometabolic risk factors among children and adolescents in a rural community in Ondo, Southwest Nigeria. J Trop Pediatr 2020;66(4):366–76. [CrossRef]
[Pubmed]
30.
Bell CS, Samuel JP, Samuels JA. Prevalence of hypertension in children. Hypertension 2019; 73(1):148–52. [CrossRef]
[Pubmed]
31.
Sundar JS, Adaikalam JSM, Parameswari S, Valarmarthi S, Kalpana S, Shantharam D. Prevalence and determinants of hypertension among urban school children in the age group of 13-17 years in, Chennai, Tamilnadu. Epidemiol 2013;3:130. [CrossRef]
32.
Karatzi K, Protogerou AD, Moschonis G, et al. Prevalence of hypertension and hypertension phenotypes by age and gender among schoolchildren in Greece: The healthy growth study. Atherosclerosis 2017;259:128–33 [CrossRef]
[Pubmed]
33.
Aldrovandi GM, Lindsey CJ, Jocobson DL, et al. Morphologic and metabolic abnormalities in vertically HIV-infected children and youth. AIDS 2009;23(6):661–72. [CrossRef]
[Pubmed]
34.
Kuciene R, Dulskiene V. Associations between body mass index, waist circumference, waist-to-height ratio, and high blood pressure among adolescents: A cross-sectional study. Sci Rep 2019;9(1):9493. [CrossRef]
[Pubmed]
35.
Kovacs VA, Gabor A, Fajcsak Z, Martos E. Role of waist circumference in predicting the risk of high blood pressure in children. Int J Pediatr Obes 2010;5(2):143–50. [CrossRef]
[Pubmed]
36.
Burgos MS, Burgos LT, Comargo MD, et al. Relationship between anthopometric measures and cardiovascular risk factors in children and adolescents. [Article in Portuguese]. Arq Bras Cardiol 2013;101(4):288–96. [CrossRef]
[Pubmed]
37.
Ewald DR, Haldeman LA. Risk factors in adolescent hypertension. Glob Pediater Health 2016; 3:2333794X15625159. [CrossRef]
[Pubmed]
38.
Salman Z, Kirk GD, Deboer MD. High rate of obesity-associated hypertension among primary schoolchildren in Sudan. Int J Hypertens 2010;2011:62949. [CrossRef]
[Pubmed]
39.
Sarfo FS, Nichols M, Singh A, et al. Characteristics of hypertension among people living with HIV in Ghana: Impact of new hypertension guideline. J Clin Hypertens (Greenwich) 2019;21(6):838–50. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
David Agatha N - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gbaja-Biamila Titilola A - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Odubela Oluwatosin O - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Musari-Martins Tomilola E - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ezemelue Priscilla N - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Opaneye Babasola A - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Lagunju Mofeoluwa M - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Arije Doyinsola M - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Abubakar Rufai A - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ezechi Lilian O - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Salako Abideen O - Conception of the work, Design of the work, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
AcknowledgmentsOur sincere appreciation to adolescents attending the ART clinic at the Nigerian Institute of Medical Research, Yaba, Lagos for their cooperation and continued trust to provide comprehensive medical care. Appreciation to the nurses, pharmacists, counsellors, and record officers of the clinic.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 David Agatha N et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


